



The bar has been raised
Reference the 2026 AHA/ASA stroke guidelines across your network.
Watch experts address key updates and their impact on care pathways in these short clips.
.png)
Summary of updates and IVT and EVT impact 
Watch 1:20
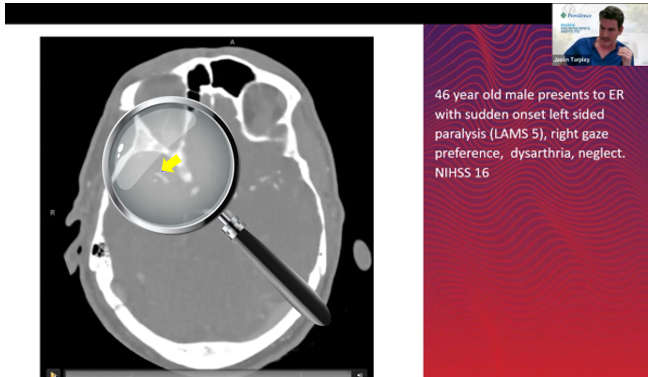
"Needle in a haystack"
MeVO detection
Watch 0:49
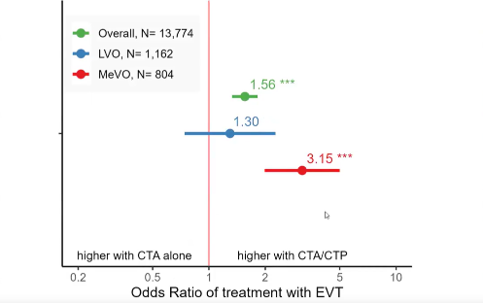
CTA vs CTP: impact on EVT procedure volume
Watch 3:04
Practical imaging workflow: CTP for all patients
Watch 3:30
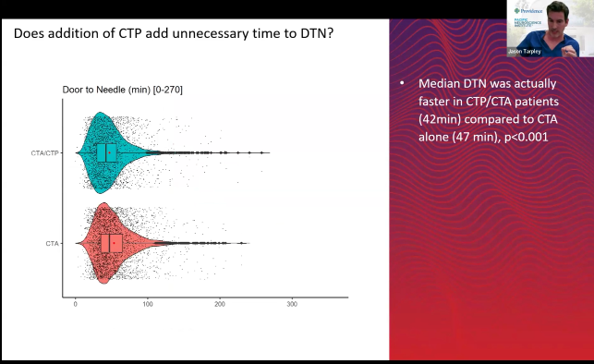
Faster times: door to needle | groin
Watch 0:39
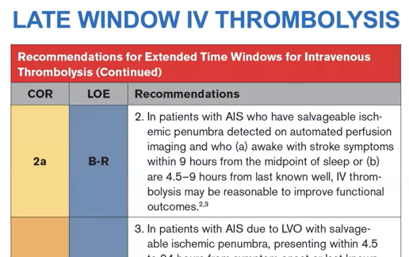
Late window IV thrombolysis
Watch 1:15
Key updates at a glance
Thrombolysis
EVT
Perfusion
Potential reimbursement

Extended window
Guidelines now support IV thrombolysis out to 9 hours from last known well — and up to 24 hours for patients with LVO who are not eligible for EVT — when advanced imaging confirms a favorable perfusion mismatch profile.
Selection is based on automated CTP or MR perfusion mismatch criteria: a penumbral volume of at least 10 mL and 20% or more mismatch.
TNK now equal to tPA
The 2026 guidelines formally recognize TNK (tenecteplase) as equivalent to alteplase for patients presenting within 4.5 hours, validating the significant transition already underway across stroke programs.
The single-bolus convenience of TNK has driven widespread adoption, and guideline equivalence now removes any remaining hesitation for programs still using alteplase as their default.

ASPECTS for large-core EVT
Now acceptable for large-core EVT eligibility, with strict score and time cutoffs.
The guidelines support EVT selection in patients with ASPECTS 3–10, expanded from the previous threshold of 6–10.
MeVO EVT
For proximal non-dominant or co-dominant M2, distal MCA, ACA, and PCA occlusions, EVT is not recommended to improve functional outcomes; a notable and somewhat controversial addition given evolving trial data.
Basilar occlusion
There is now a strong recommendation for EVT in patients with basilar artery occlusion (BAO) presenting within 24 hours, making reliable posterior circulation detection more clinically consequential than ever. These patients often present atypically, and standard LVO detection alone is insufficient to consistently identify BAO.

Standard of care
Clinically validated as standard of care across the ischemic stroke pathway — not only for late-window thrombolysis selection, but for every patient presenting with suspected stroke.
Perfusion adds meaningful value in three areas the guidelines reinforce:
-
Identifying stroke mimics that appear identical to acute stroke on standard imaging
-
Detecting medium vessel occlusions frequently missed on CTA, where perfusion helps localize the occlusion and characterize the core
-
Guiding large-core EVT decisions, where mismatch data distinguishes patients likely to benefit from those at risk of harm. For late-window patients, the guidelines are explicit — perfusion imaging is required is required for 4.5-9 hr IVT eligibility.
Standardize stroke care across your network
Reducing door-to-treatment time, ensuring appropriate transfers, and expanding equitable access to care — these are the goals that define modern stroke programs. But achieving them requires more than isolated point solutions at individual sites.

RapidAI delivers the only stroke imaging solution that supports the entire patient journey—bringing every stage of imaging and treatment into a single AI-driven platform. From acute stroke-ready hospitals to comprehensive centers, every site operates with the same level of intelligence and insight.
The result: standardized care across the network, faster and more confident clinical decisions, and fewer patients lost to variability, delays, or gaps in coverage.
Complete vessel visibility: Supporting better detection, decisions, and outcomes
Stroke doesn't limit itself to the anterior circulation, and neither should your AI.
Rapid LMVO detects suspected vessel occlusions across the ICA, MCA, ACA, Basilar, and PCA — giving your teams complete visibility into vascular pathology, not just large vessel occlusions. That means:
-
27% more stroke patients triaged compared to LVO-only detection
-
29% fewer false positives to cut through notification fatigue