


.png?width=1200&height=627&name=BLOG%20LinkedIn%20Article%20Preview%20Images%20(40).png)
Landmark stroke clinical trials DAWN and DEFUSE 3 helped validate the benefits of endovascular thrombectomy (EVT) procedure in acute ischemic stroke patients (AIS) in the late window. CT perfusion (CTP) aided in selecting eligible patients with a favorable perfusion profile.
Since imaging played a critical role in acute ischemic stroke patient selection in the two clinical trials, by 2019, the American Heart Association/American Stroke Association, Canadian Stroke Guidelines, European Stroke Organization, Korean Stroke Guidelines, and the Chinese Stroke Association updated to recommend advanced imaging for EVT patient selection and triage, especially in the late window.
The new guidelines led to discussions on the accessibility of advanced imaging and CTP and whether primary stroke centers must perform CTP on suspected large vessel occlusion patients before making transfer decisions. It also raised questions on whether CTP is too restrictive for patient selection, potentially excluding patients who could otherwise benefit from EVT.
CT Perfusion versus Non-contrast CT for Late Window Thrombectomy
Given the recent discussions on the suitable imaging modality for EVT patient selection, studies have attempted to compare patient selection using CTP and non-contrast CT (NCCT) for EVT in late-window large vessel occlusion patients. However, the results have not been consistent.
Dr. Hassan Kobeissi and co-authors performed a systemic review and meta-analysis, pooling data from five studies using CTP and NCCT to select patients for EVT. In their data analysis from 3,384 patients, although functional recovery (mRS 0-2) was comparable for patients selected by CTP and NCCT (OR= 1.03, 95% CI, 0.87-1.22; P-value= 0.71), patients selected by CTP had lower mortality rates (OR= 0.79, 95% CI, 0.65-0.96; P-value= 0.017) and higher rates of successful reperfusion (OR= 1.31, 95% CI, 1.05-1.64; P-value= 0.015).
Dr. Hassan Kobeissi and co-authors concluded that although the systemic review findings suggest that NCCT may be a valid alternative to CTP when evaluating EVT eligibility in the late window, data is limited. Prospective and randomized studies comparing CTP and NCCT are needed to confirm this possibility.
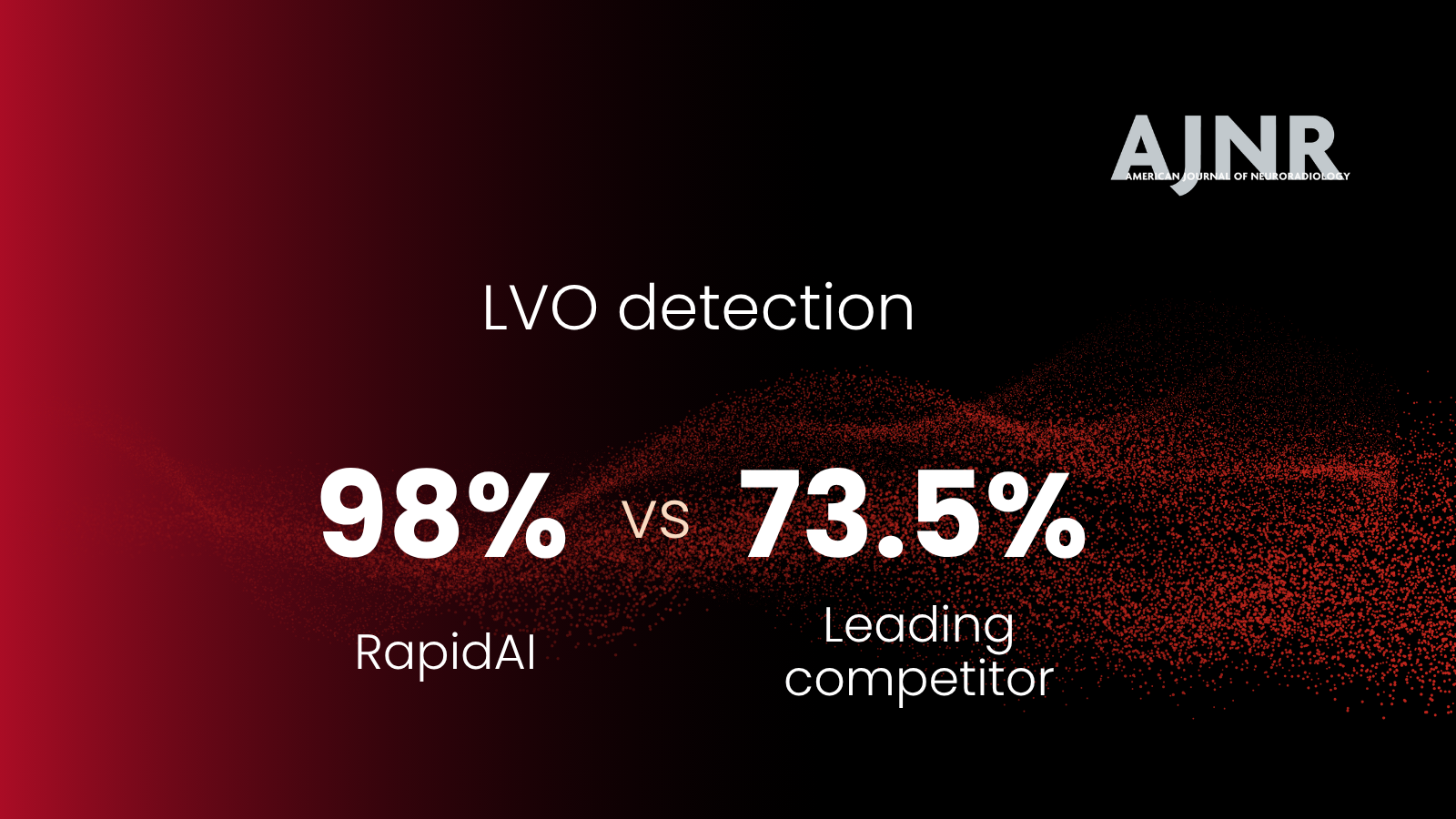
RapidAI continues to improve stroke care globally
RapidAI is committed to empowering physicians to make faster decisions for better patient outcomes, leading the next evolution of clinical decision-making and patient workflow. We’re proud to have partnered with hospitals across the U.S. to support the pivotal DAWN and DEFUSE 3 trials. We also offer a suite of NCCT solutions, giving centers of all levels greater access to quick clinical decision-making, improved patient workflow, and stroke care.