


Rapid ICH 3.0 and Rapid Hyperdensity represent the best-in-class hemorrhagic solutions supporting clinicians managing intracranial hemorrhage (both hemorrhagic stroke and head trauma). Two studies presented at the International Stroke Conference (ISC) 2023 provide further clinical evidence of the value of these technologies.
The studies were conducted by Dr. Anirudh Sreekrishnan (from Neurology & Neurological Sciences, Stanford Medicine) and co-authors and was presented by Dr. Anirudh Sreekrishnan at ISC.
Rapid ICH 3.0 essentially eliminates false positives.
With all its updates and enhancements, the latest version of the Rapid ICH software (version 3.0) accurately detects hemorrhages, eliminating false positive detections.
False positive findings can disrupt stroke workflow and cause notification fatigue.
Non-contrast CT (NCCT) scans from 900 patients were included in this study. Two expert radiologists agreed that half of these scans did not have hemorrhages, and half the scans had hemorrhages.
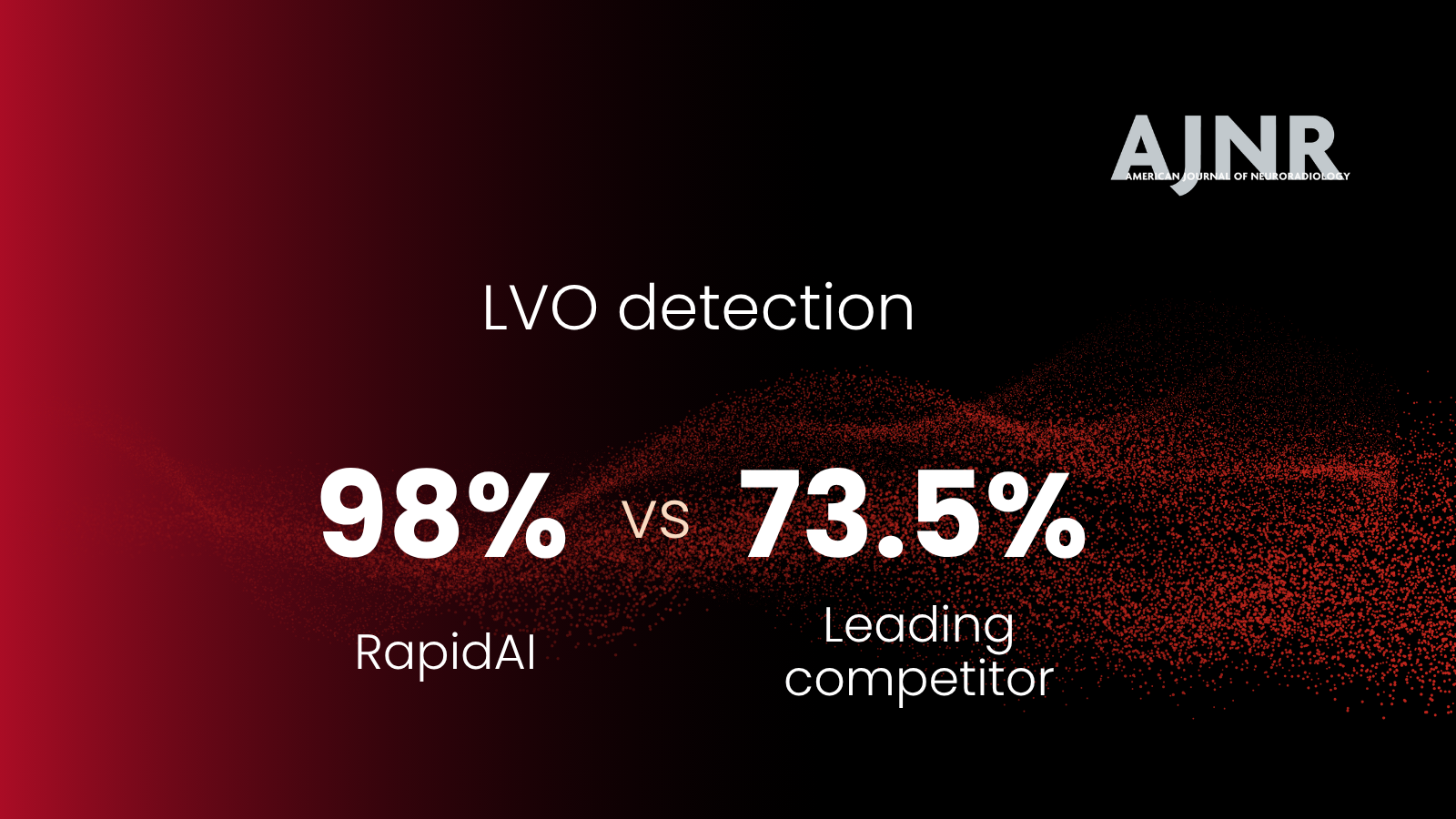
Rapid ICH 3.0 had high sensitivity and specificity of 97.84% and 99.52%. The positive predictive value was 99.56%, and the negative predictive value was 97.65%.
Rapid ICH 3.0 essentially eliminated false positives with its high specificity. It can detect hemorrhages as small as 0.4 ml, provides results in just 1 minute, and is the best available ICH detection software in the market. Rapid ICH 3.0 also picks up all hemorrhage subtypes.
There was a high correlation between manual and Rapid Hyperdensity measurements of hemorrhage volumes.
Dr. Anirudh Sreekrishnan and co-authors examined whether Rapid Hyperdensity accurately measures hemorrhage volume by automatically quantifying and characterizing hyperdense regions >1ml on NCCT scans. They also investigated if Rapid Hyperdensity can detect changes in hemorrhage volume or ICH growth in the follow-up NCCT scan.
Expert neuroradiologists and Rapid Hyperdensity evaluated baseline NCCT and follow-up scans at 24 hours from 127 patients.
For baseline scans, there was a high correlation between manual measurements and the volumes measured by Rapid Hyperdensity (p<0.001).
For the follow-up scans, there was a high correlation between measurements of expansion for both absolute difference (p<0.001) and percentage difference (p<0.001).
ICH growth is defined as an increase of 6 cc and/or 33% in volume in the follow-up imaging. When comparing ICH growth measured by neuroradiologists and Rapid Hyperdensity, the software had a sensitivity of 94.12% and specificity of 97.27%.
Manually measuring hemorrhage volume is time-consuming. The pilot study presented at ISC 2023 highlights how Rapid Hyperdensity can quickly and accurately measure intraparenchymal hemorrhage volumes, facilitating faster team activation, standardizing volume measurements, and streamlining triage and transfer decisions.
Streamlining triage-and-transfer decision-making expedites patient care.
Rapid ICH and Rapid Hyperdensity provide contextual data critical to helping clinicians make more informed triage and transfer decisions by automatically processing non-contrast CT images and notifying clinicians of the findings.
Rapid ICH 3.0 assesses the scans for all hemorrhage subtypes, including intraparenchymal (IPH), intraventricular (IVH), subdural (SDH), and subarachnoid (SAH) subtypes, then, if detected, immediately notify clinicians of the suspected intracranial hemorrhage (ICH).
Check out our latest Rapid ICH 3.0 and Rapid Hyperdensity modules.