


Radiology is in a strange moment. The profession has never been more essential, yet trainees still hear: "AI is coming for radiologists." Meanwhile, imaging volumes keep climbing and radiologists are being asked to do more with less.
The biggest risk to the radiology workforce is not AI replacing radiologists—it's radiology losing control over how AI is adopted, how workflows are designed, and how the next generation is trained. When those decisions are made without radiologist leadership, AI can add complexity and increase cognitive burden. This is a systems issue rooted in governance and design.
In Episode 3 of Radiology Rewired, Dr. Vivek Singh explores this reality with Dr. Dhairya Lakhani (West Virginia University) and Dr. Vivek Yedavalli (Johns Hopkins). Their message: radiology's future depends on radiologists embracing AI on their terms, with guardrails that protect clinical judgment, strengthen training, and reduce burnout.
The real threat is losing control of how radiology is practiced
Radiology workforce strain is not theoretical. Professional organizations warn about the widening gap between imaging demand and radiologist supply, with downstream effects on access and timeliness of care.
The practice environment has shifted. Autonomy has become less common, replaced by hospital employment and large groups. This contributes to a feeling many radiologists recognize: less control over workload and fewer levers to improve daily experience.
If radiologists don't lead AI adoption and workflow governance, they risk becoming reactive to decisions made elsewhere. That's how technology adds clicks and cognitive burden without fixing real constraints.
Why "AI will replace radiologists" still harms the pipeline
Even as radiology remains highly in-demand, the perception problem persists. Public narratives simplify radiology to "image interpretation," ignoring that radiologists are consultants and core care team members.
This has measurable impact. When students believe radiology jobs are at risk, they choose other specialties, even as imaging demand rises.
Episode 3 makes a key point: AI is not why radiology will struggle to recruit; misunderstanding radiology's value is. If the profession doesn't educate trainees and the public, the pipeline problem gets worse.
The core truth: the future workforce depends on radiologists owning AI adoption
The most useful line from the episode: Radiologists who use AI well will outpace radiologists who don't. But that means building an environment where AI augments clinical expertise rather than displacing clinical thinking.
What "owning AI adoption" actually means
- Radiologists have a seat at the table when tools are selected
- Tools are assessed against real workflow pain points
- Leaders track downstream impact on time-to-diagnosis and reading-room burden
- Radiologists define where AI outputs belong to reduce friction
Without this discipline, AI creates new work. Real-world adoption shows "workload reduction" is not automatic.
Cognitive offloading is the training risk leaders need to address now
Episode 3 highlights a real risk for residency training: cognitive offloading, where trainees rely on AI as the primary interpreter rather than as a second reader.
This has safety implications. Radiologists need to know when AI is wrong, and that requires fundamentals: anatomy, pattern recognition, and clinical reasoning.
Practical guardrails that protect clinical judgment
- Use AI to surface relevant context and findings early
- Interpret the study with that context in mind
- Validate, refine, and synthesize the final impression independently
This keeps AI augmenting expertise, not replacing interpretation.
What sustainable AI adoption looks like in real workflows
Episode 3 gives examples of where AI genuinely supports the radiology workforce by improving clarity and triage.
1. Worklist prioritization that protects patients and radiologists
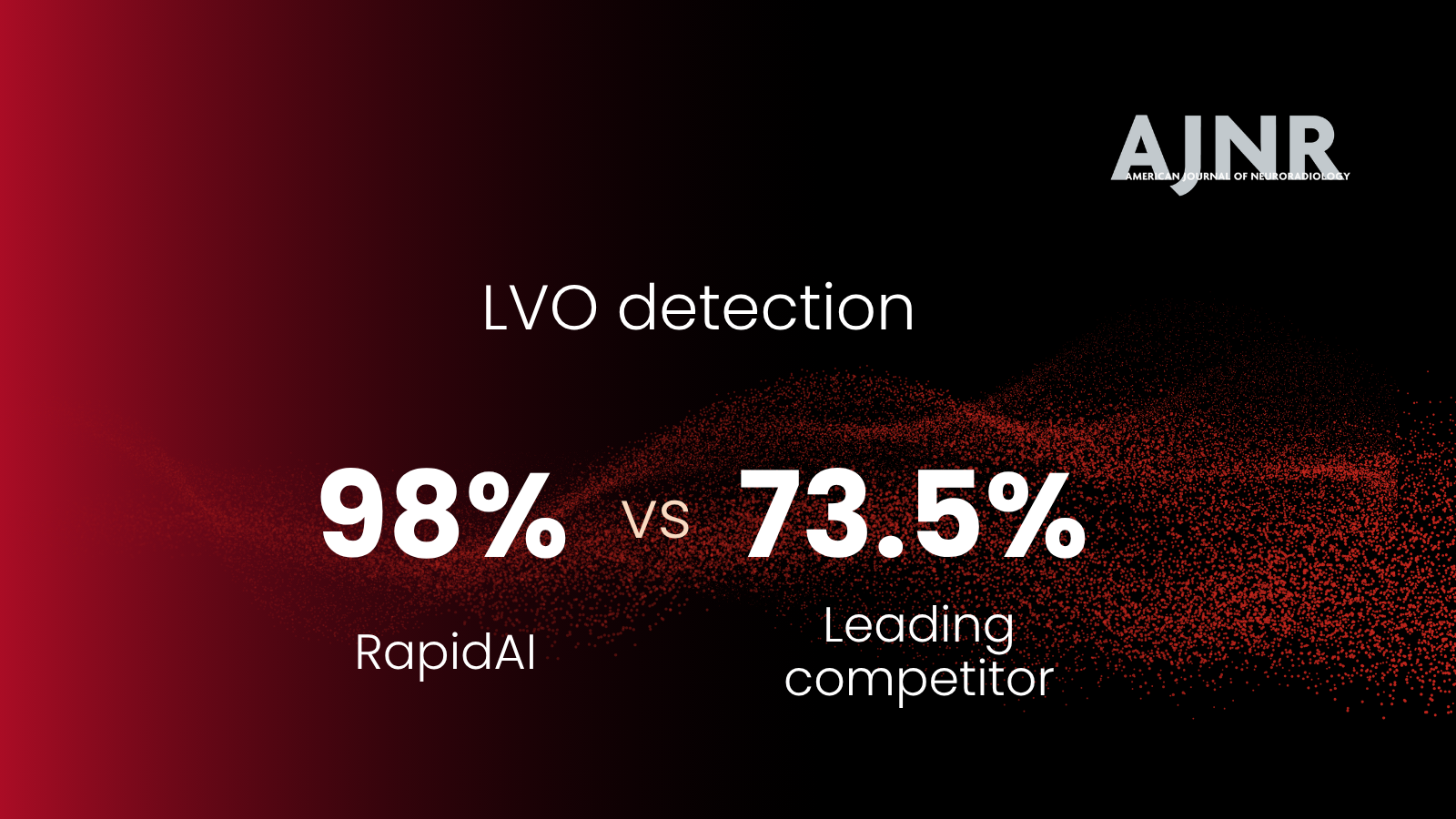
Clinical AI that flags potential acute findings helps ensure time-sensitive cases rise to the top. This reduces the mental tax of deciding what to read first.
2. Better histories, better reads, fewer delays
AI can improve the quality of clinical information delivered to radiologists. Better context supports better decisions and fewer downstream clarifications.
3. AI that removes repetitive steps and preserves cognitive bandwidth
Radiologists want AI to:
- handle repetitive measurements
- reduce tedious reconstruction steps
- standardize structured reporting components
- reduce time spent hunting for details
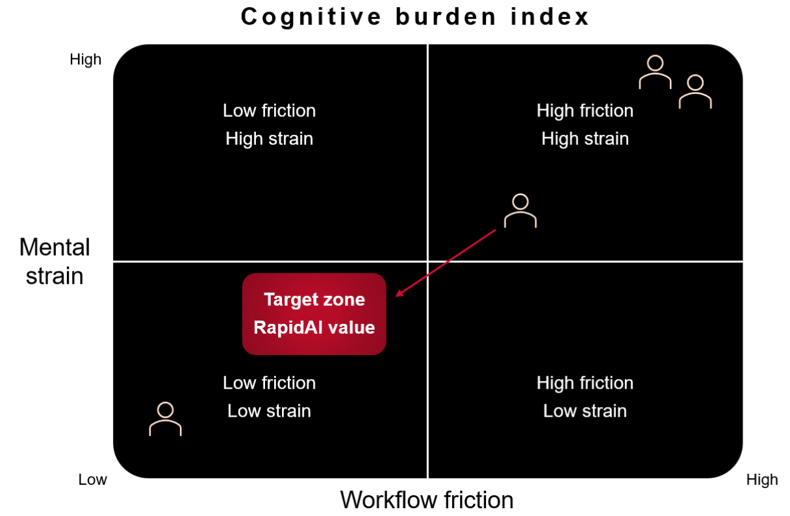
For more on workflow friction: See reducing cognitive burden in radiology.
To see how RapidAI approaches radiology workflow:
Explore RapidAI radiology solutions
For AI-supported acute triage:
See RapidAI neurovascular solutions
What leaders can do this year to protect the future radiology workforce
AI strategy is workforce strategy. Here's a practical leadership checklist:
- Create an AI governance path that includes radiologists
- Evaluate tools against one standard: do they reduce friction?
- Protect training from cognitive offloading with "read first, verify second"
- Focus on systems, not point solutions
- Reframe the narrative for medical students about radiology's consultative value
Listen to the full conversation
To hear Dr. Vivek Singh's full discussion with Dr. Dhairya Lakhani and Dr. Vivek Yedavalli, listen to Episode 3 of Radiology Rewired.
Listen to Radiology Rewired: Episode 3 YouTube | Apple Podcasts | and Spotify
FAQs
Will AI replace radiologists?
No. AI can automate repetitive tasks and support detection and triage, but radiologists remain responsible for clinical synthesis, context, communication, and judgment. The larger risk is adopting AI without guardrails that protect training and workflow quality.
What is cognitive offloading in radiology?
Cognitive offloading is when trainees or clinicians rely too heavily on AI outputs and stop doing the independent thinking required to interpret images. It can reduce skill development and increase risk when AI is wrong.
How does AI help the radiology workforce today?
AI can support worklist prioritization, reduce repetitive measurements, improve access to clinical context, and streamline communication. The most meaningful benefits come from integrated systems that reduce workflow friction and cognitive burden.
What should residency programs do as AI becomes more common?
Residency programs should train residents to interpret independently first, then use AI as a second reader. Programs should also teach AI strengths and limitations so trainees learn how to verify outputs and recognize failure modes.
How can hospitals make AI adoption support workforce sustainability?
Hospitals should implement AI with radiologist-led governance, measure real workflow impact, prioritize integrated solutions, and protect training from over-reliance on automation.
578-MKT-Web-0126